Water/wastewater
Published over 5 years ago. See the latest and most current information on Water/wastewater.
The majority of 4,000 odd pharmaceutical products on the market globally have not been assessed for their occurrence, environmental fate or environmental impacts. Studies around the world have found pharmaceuticals present in surface waters at concentrations of concern. This is perhaps not surprising as the use of medicines is increasing for various reasons in western countries. Indeed, the current Covid 19 pandemic has contributed a further increase in the use of medicines, particularly antibiotics. So which substances are present in water and at what kind of concentrations? What methods are available to monitor pharmaceuticals, their metabolites and other emerging contaminants at the limits of detection necessary to ensure that no biological effects are predicted? How do they enter surface waters? And how can they be better managed to prevent impacts on the environment and human health?
The presence of pharmaceuticals in the water environment is of concern as they are designed to produce a biological response at a very low dose. They are tailored to be stable (or ‘persistent’) to interact with target molecules. These qualities mean that pharmaceuticals therefore can have unintended impacts in the environment. The main effects are seen in aquatic life; for example, the well-publicised feminisation of fish from exposure to oestrogenic substances which can lead to population collapse, also Fluoxetine (Prozac) is also known to alter fish behaviour and affect their survival and reproduction success. Another significant impact is an increase in antimicrobial resistance due to the widespread presence of antibiotics in the environment. There are already 700,000 deaths per year due to antimicrobial resistance, according to the World Health Organisation, but this is predicted to rise to 10 million deaths per year by 2050 if nothing is done. Another cause for concern is the lack of human risk assessment regarding long term and low levels of exposure to pharmaceuticals, especially in sensitive populations such as pregnant women, foetuses and children, stresses Sharon Pfleger, Consultant in Pharmaceutical Public Health. According to the European Environment Agency, human exposure to pharmaceuticals is known to cause thyroid disease, increased cholesterol levels, liver damage, kidney cancer, testicular cancer, and developmental effects on the unborn child with other effects suspected but not yet proven.
“Medicine use is increasing for a number of reasons”, explains Sharon Pfleger, “Such as growing and ageing populations, technological advances, and a ‘pill for every ill’ culture.” According to Ms Pfleger, a typical 80-85 year old consumes 20 times as many medicines as a 20-25 year old.
In terms of regulation, drinking water quality standards in Europe have been established by the Drinking Water Directive (DWD) (98/83/EC) which set out “to protect human health from adverse effects of any contamination of water intended for human consumption” by ensuring that it is “wholesome and clean”. Under the original DWD, a total of 48 microbiological, chemical and indicator parameters had to be monitored and tested regularly. This Directive has been revised and a new DWD was ratified in October 2020, to be transposed into member state legislation within 2 years. Amongst the changes are stronger catchment risk assessments (linked with the Water Framework Directive requirements), longer lists of parameters for measurement (bisphenol A must now be monitored) and new ‘watch lists’ for potential emerging contaminants such as endocrine disrupting chemicals, pharmaceuticals, plastics and new chemicals in the supply chain. ”The first watch list will be published in 2021 and will include 17β-estradiol and nonyl phenol,” explains Moira Malcolm, Drinking Water Specialist at the Drinking Water Quality Regulator, Scotland, “Watch lists will be produced regularly as emerging chemicals are identified and measurement techniques become available, so there will be a greater need for monitoring”. (Scotland has committed to keep pace with changes in EU Directives after Brexit.) Ms Malcolm points out that according to Drinking Water Inspectorate research, pharmaceuticals were not present in 2011 in concentrations of concern in drinking water.
Case study: Monitoring commonly occurring pharmaceuticals in the River Ugie
The River Ugie is categorised as a priority catchment to achieve ‘Good Ecological Status’ under the Water Framework Directive, and is used by Scottish Water as a drinking water source for Aberdeen. Zhang et al (2018) selected 6 pharmaceuticals and personal care products (PPCPs) from a list of PPCPs commonly present in the aquatic environment around the world (Diclofenac, Ibuprofen, Paracetamol, Tramadol, Carbamazepine, Triclosan).
PPCPs were monitored monthly over a year using a combination of spot sampling (and laboratory analysis using GC-MS after derivatisation) to validate results from passive sampling using a Polar Organic Chemicals Integrated Sampler (POCIS). The cumulative passive sample collected from the POCIS was subjected to solvent extraction and chemical recovery and then chemical analysis also using GC/MS after derivatisation. Overall, results from passive sampling were in good agreement with spot sampling results.
In this remote rural river, all 6 of the PPCPs were detected; Carbamazepine and Ibuprofen were on average the dominant contaminants. The highest recorded concentrations were 192.7 ng/l for Carbazamepine and 119.4 ng/l for Paracetamol. In general the highest concentrations of the 6 determinands were found at a site closest to a wastewater treatment plant and near the largest village in the catchment, which is likely due to wastewater effluent and use of pharmaceuticals. The levels detected were similar to those observed in other European countries.
An ecological risk assessment was undertaken by Zhang et al by calculating a risk quotient for each substance, by dividing the quantity present by the toxicity of each (using the predicted no effect concentration). For the 6 substances, Triclosan was deemed to be of medium risk, the others were low or minimal risk to the aquatic environment due to the quantities present and toxicity of each.
Monthly and annual outflows of the 6 substances into the Ugie Estuary and the North Sea were also estimated. The total annual outflows were estimated to be 4.6 kg. Following this, the researchers wondered what quantity of these 6 substances must be discharged globally into the sea? Their ballpark calculations suggest this could be as much as 1,383 tonnes per year globally, a staggering amount just for these 6 substances, without taking into account other pharmaceuticals and chemicals being leached into the sea. Toxicological research is only just starting to consider the combined effects of exposure by organisms to multiple substances simultaneously.
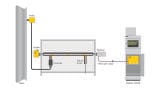
The key sources of pharmaceuticals and their metabolites in the environment are consumption and excretion into the wastewater system, inappropriate disposal down sinks and toilets, and from the manufacturing industry (image 1). After passing through the human or animal body, medicines are excreted either in an unchanged active form or as metabolites, which may be active or inactive, and have the potential for further breakdown into numerous transformation products in wastewater treatment plants (WWTPs) or in the environment.
However, conventional WWTPs are not 100% effective in removing emerging contaminants including pharmaceuticals and their metabolites (image 1). Studies around the world have found pharmaceuticals present in water bodies (image 2). Globally 631 pharmaceuticals and metabolites were found in the environment in a combined study by aus der Beek in 2015. Residues of 16 pharmaceutical substances were detected in the surface, drinking, and groundwater of all the UN regions. These substances do not necessarily reflect the most commonly present pharmaceuticals as the reasons for the detection of these substances depend on prioritisation of substances for monitoring and resources available in each country. The 16 substances detected included: Diclofenac (anti-inflammatory), Carbamazepine (epilepsy drug), Ibuprofen, Sulfamethoxazole (antibiotic), Naproxen (anti-inflammatory), Estrone (oestrogen steroid/hormone), Estradiol (oestrogen steroid/hormone), Ethinylestradiol (synthetic oestrogen used in the pill for birth control), Trimethoprim (antibiotic), Paracetamol, Clofibric acid (metabolite of a cholesterol lowering drug), Ciprofloxacin (antibiotic), Ofloxacin (antibiotic), Estriol (steroid/hormone used in hormone replacement therapy), Norfloxacin (antibiotic) and Acetylsalicylic acid (aspirin).
What kind of concentrations of pharmaceuticals are found in the environment? A study in 2019 (Boxall and Wilkinson) found antibiotics present in river samples from 65% of sites in 72 countries. 111 of 711 sites had antibiotics above the safe threshold; in the worst cases at levels 300 times the limit set by the Antimicrobial Resistance Industry Alliance. Rout et al (2021) found emerging contaminants in wastewater treatment plant effluent at up to 850 ng/l (Iopromide used as a contrast medium in radiography) and in sewage sludge at up to 4,800 ng/g (Ciprofloxacin, an antibiotic). Even in a remote rural river in Scotland, the River Ugie, Carbamazepine and Ibuprofen were present at an average of 11.23 ng/l and 13.06 ng/l respectively (Zhang et al, 2018).
Taking one example, the predicted no effect concentration for ecotoxicity for Ciprofloxacin is 1200ng/l – the concentration found in sewage sludge (by Rout et al, 2021) was above this threshold; if the same concentrations were found in the environment they would be expected to cause toxicological effects on aquatic ecology. Dr Zulin Zhang, Senior Environmental Scientist at the James Hutton Institute explained that reproductive effects caused by pharmaceuticals present in quantities as low as parts per billion (ppb). Therefore, highly sensitive technologies that can measure down to ppb or even parts per trillion (ppt) are needed. However, Dr Zhang says that pharmaceuticals are notably difficult to measure, despite concerns over their relatively significant environmental impacts monitoring techniques need further advancement.
“The environmental occurrence and detection of emerging contaminants has really only been investigated over the last 20 years”, explains Richard Luxton, Director or the Institute of Biosensing Technology at the University of the West of England. Historically chromatography laboratory methods have been used to detect emerging contaminants, but there are now sensors and biosensors under development to detect these substances in the field. The advantage of chromatography is that it can detect the presence of unknown substances, whereas sensors must be developed to recognise and detect specific substances. “The two methods can be used to complement each other”, says Professor Luxton, “with chromatography methods being used to confirm the presence of target pharmaceuticals in water samples and the sensors being used to detect and monitor target substances of concern over time”.
A review of papers on new sensing technologies for emerging contaminants showed that about 25% are based on optical measurement whereas approximately 75% use electrochemical measurement (voltammetry, amperometry, impedance sensing and Field Effect Transistors) and around 1% are based on thermal sensors. Examples include a highly sensitive electrochemical graphene-based aptasensor developed to detect 17β-estradiol, using a unique, folded DNA molecule on the sensor surface to capture and detect estradiol, with a limit of detection (LOD) of 2.7 × 10-3 ng/l (Liu et al, 2019). Another new technology is a Molecular Imprinted Polymer (MIP) sensor to detect 17β-estradiol which is even more sensitive with an LOD of 1.7 x 10-3 ng/l. These represent technologies which can detect substances at ppt but Professor Luxton questions whether this level of sensitivity is always needed “sometimes presence or absence of a substance is enough from a field sensor and then lab analysis of a water sample can be used to confirm the quantity” explains Professor Luxton.
The next technological step is to link sensors for pharmaceuticals with a smartphone app to display results for in situ water quality monitoring. Integrated systems like this are under development, for example to measure a combination of acetaminophen (pain killer) and 17β-estradiol, and the heavy metal, lead using a potentiostat connected to three multiwalled carbon nanotubes and β-cyclodextrin screen printed electrodes (Alam et al, 2020).
Case study: Caithness General Hospital achieves the AWS International Standard for Water Stewardship
This pilot study was conducted to assess the effects of the Caithness General Hospital (CGH) on pharmaceutical pollution in Wick wastewater, and to monitor the changes in water quality as it travels from the drinking water source to the hospital and receives treatment at Wick WWTP (Niemi et al, 2020).
Sampling was carried out every day (morning or afternoon) over four weeks at Loch Calder (drinking water source), the hospital (kitchen tap water and combined wastewater outflow) and Wick WWTP (raw influent and final effluent) to investigate temporal trends in pharmaceutical concentrations. Over the 28-day study, 20 sampling events were performed for the hospital wastewater, 19 for the Wick WWTP influent and effluent and 4 for the Loch Calder source water and hospital tap water.
Water quality analysis was carried out following in-house procedures developed for research and commercial work. For pharmaceutical analysis, a solid phase extraction method and liquid chromatography-tandem mass spectrometry (LC/MS/MS) analysis technique were developed to monitor select compounds from four pharmaceutical classes: three analgesics and anti-inflammatories (paracetamol, diclofenac and ibuprofen), two antibiotics (clarithromycin and trimethoprim), two psychiatric drugs (carbamazepine and fluoxetine) and a synthetic hormone (17α-ethynylestradiol). Several of these compounds are controlled under UK and European water quality legislation due to their properties. Understanding the fate and transport of these compounds in wastewater and the receiving environment is therefore a priority.
NHS Highland worked in partnership with a number of agencies including the Scottish Environment Protection Agency, Scottish Water, Highland and Islands Enterprise and the University of the Highlands and Islands’ ERI in Thurso. The partnership, known as the One Breakthrough Partnership, is working to improve water quality, reduce the environmental impact of healthcare, reduce pharmaceutical wastage (e.g. through an educational campaign), reduce costs, and create integrated healthcare (green prescribing and lifestyle changes to reduce prescriptions). An early warning system is being investigated to link prescribing data with Scottish Water monitoring data so that the water company and environmental regulator could have advance warning of the quantity of medicines that will need treatment downstream and linking with SEPA to identify when extra environmental monitoring may be needed.
In 2020 Caithness Hospital was the first hospital in the world to achieve the AWS water stewardship standard, and the only site in the UK to achieve this standard. The project hopes to achieve multiple benefits including reduction of water, energy and carbon footprints for water treatment and ultimately that the pill for every ill culture moves to a more preventative one.
Another approach is to remove pharmaceuticals from water by selectively adsorbing them to a surface. A European project (RECOPHARMA) is looking at removing cytostatic drugs (CDs) which are persistent in the environment and known to be present in effluent from urban wastewater treatment plant and hospital effluent across the world. CDs have been detected in wastewater effluent in concentrations up to 146 ng/l for Cyclophosphamide and up to 200 ng/l for Tamoxifen for example. Certain CDs are difficult to remove from water using standard wastewater treatment methods and are transferred to surface water with unknown effects on the environment. MIPs (see above) have been developed to selectively adsorb and treat such CDs so that precious raw materials employed for their production can be recovered and actually reused to create a closed loop cycle.
“Going forward there is definitely an opportunity for innovation in sensors combined with digital healthcare to provide solutions to the issue of pharmaceuticals in the environment”, says Sharon Pfleger. According to Ms Pfleger, better management of pharmaceuticals in the water environment will require:
• Measurement of the occurrence, fate and impact of more medicines in the environment;
• A better understanding of the effects of a mixture of medicines compared with effects of a single medicine;
• Monitoring the effects of metabolites and transformation products;
• A better understanding of different routes of exposure;
• The presence of pharmaceuticals in treated versus untreated waters (septic tanks);
• Identification of common indicator substances;
• Standardisation of data collection, quality and storage; and
• Prioritisation of contaminants, water bodies and ecosystems for monitoring.
IET 36.3 May